
Osteoarthritis is the most common joint disease affecting elderly population. Almost 15-20% of people more than 55 years of age can have symptomatic knee OA. It commonly affects knee or hip joints and presents as joint pain and crepitus in the knee.It is also the leading cause of disability worldwide.
What is OA?
- OA is the most common joint disease affecting human beings and an important cause of disability
- Knee and hip joints are commonly affected
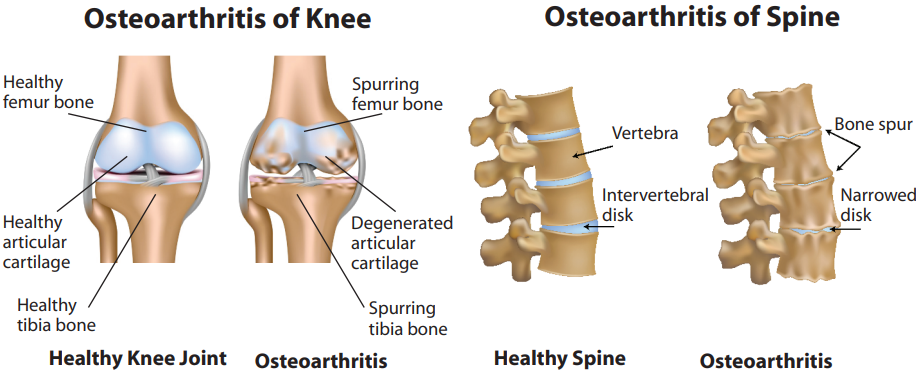
- There is a focal loss of cartilage
- Body attempts to form a new bone- osteophyte
- Inflammation of joints covering called synovitis
- Leads to pain and joint swelling
OA in Males & Females
- IN FEMALES
More extensive involvement More symptoms Increased prevalence of knee and hand joint - IN MALES
Hip Involvement Secondary OA
Symptoms
- Persistent knee pain originates from capsules, synovium, periosteum, ligaments etc.
- Pain increases when standing, climbing up the staircase or walking
- Difficulty in squatting for toilet
- Catch like sensation while climbing down the staircase or knee locking
- Night pain in knees can be disturbing
- Morning stiffness of knee lasting for 5 – 30 min
Common risk factors for osteoarthritis of knee & hip
- Age greater than or equal to 50 years
- Obesity (knee osteoarthritis)
- Being female (especially for knee osteoarthritis)
- Family history
- History of immobilization
- Injury to the joint
- Prolonged occupational or sports stress
What goes wrong?
Management of osteoarthritis
PHARMACOLOGICAL THERAPY
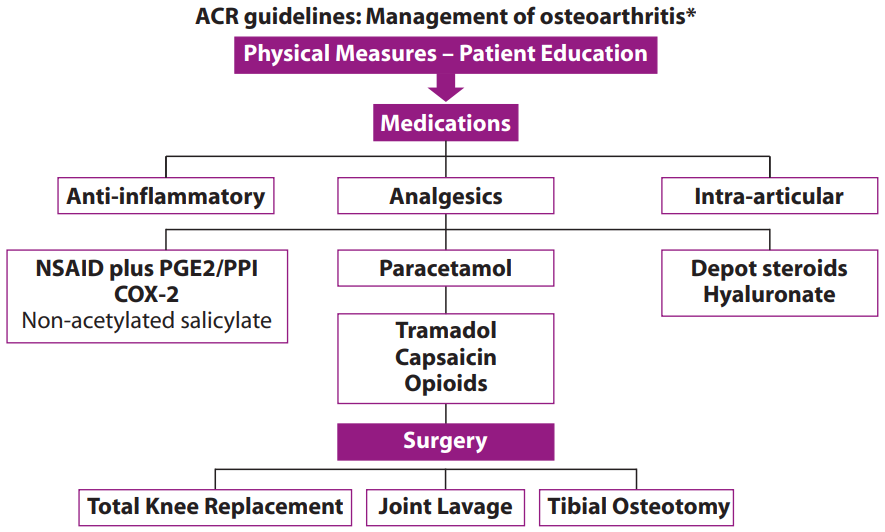
NON-PHARMACOLOGICAL THERAPY
Visco Supplementation
- Intrarticular hyaluronan injection provides symptomatic relief by 60-70% to knee osteoarthritis patients
- Chondrocyte transplant have been shown to regenerate near normal hyaline cartilage but are not routinely recommended
Surgical Management
Joint replacement must be considered in any patient presenting with end-stage joint disease
with persistent pain not responding to conventional treatments.
Total Knee Replacement (TKR) is opted by patients who are older and have weakness and
impaired extension of knee. These patients have severe difficulty in doing daily chores like
climbing up staircase and getting up from chair.
Total Hip Replacement (THR) and Total Knee Replacement (TKR) have improved quality of life
and decreased morbidity of OA.90% of patients have excellent long-term results.
The other surgical options for TKR are
- Loose body removal
- Osteotomy
- Arthrodesis
- Arthroplasty
- Synovectomy
Recent advances in OA
- Tetracycline
- 10-methyl adenosine
- Chondrocyte stem cell transplantation
- Joint lavage
ADULT CARE
Association of OA
- Age more than 55 years
- Trauma to joints
- Underlying disease of knee such as rheumatoid arthritis
- Obesity precedes OA
- Female sex
- Occupational knee bending,prolonged squatting
- Symptomatic OA increases with age
FACT
Knee OA is common in India while hip OA is common in western population.
Genetic basis of OA
- Herberden nodes in families
- 65% concordance in twins
- Associated with HLA A1, B8 @ HFE gene mutation
Why arthritis hurts?
- Damage to the joint tissues
May result from disease process or from injury,stress or pressure to the joints - Inflammation
Damaged joints swell up and become inflamed adding pressure to your nerves. - Fatigue
Can make your pain seem worse and harder to handle. - Stress or Depression
A result from the inability to move and do the activities you enjoy. Stress and depression can make managing pain and arthritis more difficult.
Signs
- Swelling and pain in knee or hand joints
- Areas affected – area of maximal we ight load. Commonly affected joints – Knee, Hip & Thumb base
- Bowing of knees seen in 50% of individuals suffering from OA
- Crepitus – sensation of bone rubbing against bone, on movement
- Restricted movement
- Deformities
- Spine pain/backache,hip pain
- Elbows/ankles/PIP are rarely involved in OA
- Hand joints OA
– Herberden’s node
– Bouchard’s nodes - Spinal OA
– Lumbar spondylosis
– Cervical spondylosis
Investigations
- X-ray of knees in standing position
– Joint space narrowing
– Osteophytes
– Subchondral bone sclerosis
– Deformities, loose bodies - CT scan for axial joints (spine)
- Ultrasound is used for assessing periarticular structures
- MRI – cartilage evaluation
How to diagnose?
Diagnosis is essentially clinico radiological
- 50% of OA by radiograph are clinically symptomatic
- Early OA can be diagnosed by MRI of knee-cartilage defects or meniscal damage
Orthotics used in OA

Shoes, Cane, Knee braces, Paraffin baths, Hot packs to relieve muscle spasm whereas Ice packs when knee is influenced