
Radical surgery intended to cure cancer tends to cause some damage to the operated organ and the subsequent quality of life of the patient. It is now a worldwide trend to preserve organ function and minimise operative damage without compromising the outcome of treatment. The organ and function preservation of the affected organ is the most rapidly progressing concept in the management of urological cancer.
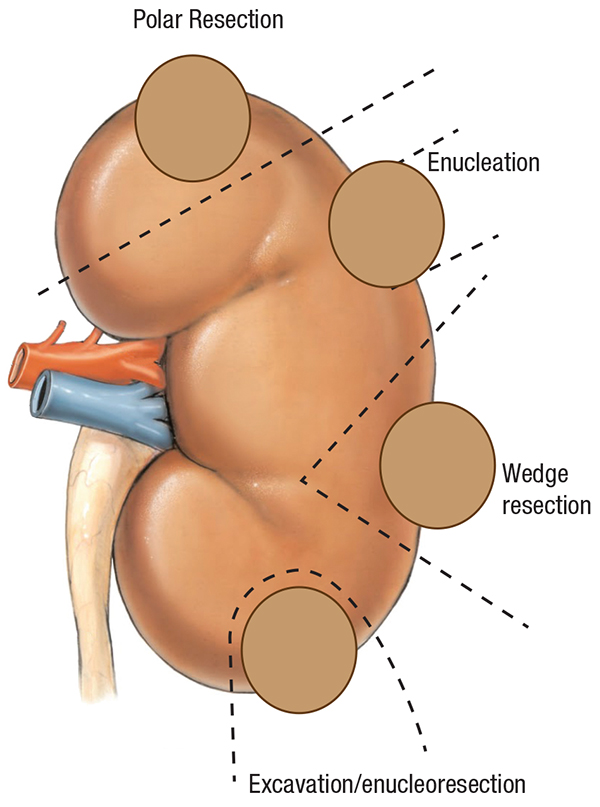
In cancer of the kidney, renal tumours less than 4-5 cm earlier had to be managed by removing the entire organ (Radical Nephrectomy). However, now kidney parenchyma preserving approaches like nephron-sparing surgery or partial nephrectomy are standard care for renal tumours. The newer methods can also be achieved using the traditional open surgery or by the laparoscopic method. Renal or nephron preservation is important as patients may develop renal insuffi ciency in the long run. Majority of patients have diabetes and hypertension, which can also damage the kidneys. Therefore, it is always advisable to preserve as much renal parenchyma as possible without compromising cancer control.
Incontinence and erectile dysfunction are the most important complications that could happen after removal of bladder (radical cystectomy) and prostate (radical prostatectomy). Today, nerve-sparing procedures (cavernous nerves) in radical cystectomy and radical prostatectomy for retaining potency are used for providing better quality of life in terms of better continence and sexual function after surgery.
In early bladder cancer, bladder is preserved by endoscopic removal of tumour and intravesical chemotherapy; in invasive bladder cancer however, radical cystectomy is the treatment of choice. New reconstructive surgeries such as neobladder (new bladder) formation using intestinal segments have been developed for recovering the lost function. Over the past decade, alternative organ preservation strategies using multimodality treatment (surgery, radiation and chemotherapy) have offered an option for bladder preservation in select patients with invasive bladder tumour.
Organ-preserving techniques in penile cancer include cold-knife excision, laser surgery and Mohs micrographic surgery; these could be done in highly select patients and avoid partial or total amputation of penis, for fear of disfi gurement and profound effect on sexual function. Testis preserving surgery is sometimes possible for tumours less than 2 cm situated in the polar region of the testes.