-for-thoracic-masses-image")
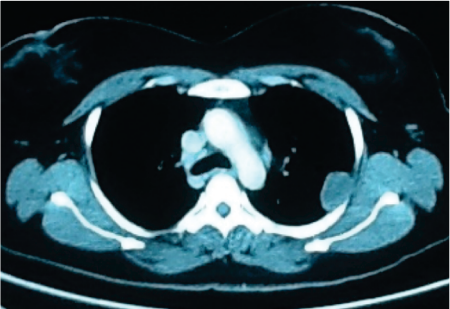
We present a case of a 43 year-old-lady, who presented with cough and left sided chest pain. The cough was dry, unresponsive to medications and the pain was not related to exertion. A Chest Radiograph and contrast enhanced CT-Chest was performed. These revealed a 3.4×2.1 cm homogenously enhancing pleural based nodule adjacent to left 3rd and 4th inter costal space. A Needle biopsy was performed which was suggestive of solitary fibrous tumor. She was advised surgical excision. After relevant investigations, she underwent Robotic Assisted Thoracoscopic Surgery (RATS).
This was performed using the Da Vinci Robotic system at our hospital. She was intubated with a double lumen endotracheal tube; she was kept in right decubitus position with left chest up. Left lung was collapsed and four ports were inserted for the procedure: two 10 mm ports for camera and assistant and two 8 mm ports for robotic arms.
A well encapsulated subpleural mass was seen arising from the third intercostal space. The parietal pleura was incised with diathermy and mass enucleated. An inter costal drain was inserted through one of the port and other port sites sutured. Patient was extubated in the operation room and shifted to her room after a few hours. The postoperative recovery was uneventful. Inter costal drain was removed the next day & the patient was discharged a day later. Final pathology confirmed the diagnosis of benign fibrous tumour. She was not offered any post operative treatment and is on regular follow up. Surgical approach for intra thoracic masses such as this can be either conventional ‘open’ surgery or video assisted thoracoscopic surgery (VATS).
The former would involve fairly large thoracotomy incision, cutting of muscles and retraction of ribs to approach the tumour. It is associated with significant post operative pain, prolonged recovery period and a large unsightly scar. Video Assisted Thoracoscopic approach avoids the trauma of open surgery. The post operative pain is significantly less, pulmonary morbidity is reduced, postoperative recovery is much faster, the length of hospital stay is shorter and surgical scars are more aesthetic.
Robotic Assisted Thoracoscopic Surgery offers all the advantages of minimal invasive surgery and scores over VATS due to the following :
- Increased magnification (x10) with 3D imaging
- Increased dexterity and articulation relative to standard rigid MIS instruments
- Seven degree of motion of robotic instruments
- Tremor filtration and motion scaling potentially aiding finer movements
- The console at which operating surgeon seats comfortably
Robotic Assisted Surgery therefore spared our patient of post operative morbidity, prolonged hospital stay and an ugly scar of thoracotomy. As surgery evolves, we know how the application of modern technology can facilitate easier transitions for surgeons towards lesser invasive surgeries, making it safer and more efficacious for the patient. Da Vinci robot is increasingly being used for complex thoracic procedures. Indications for RATS are excision thymus and thymoma, pulmonary lobectomy for early lung cancer, esophagectomy for cancer of the esophagus and mediastinal lymph node dissections.
Michael Kent form Mount Sinai Medical Centre New York in a review of national database of open, video assisted thoracic surgery and Robotic lobectomy ( Ann Thorac Surg,2014;97:236-44)concluded that ‘case volume of robotic pulmonary resection has increased significantly during the study period and thoracic surgeons have been able to adopt to robotic surgery safely. Robotic resection appears to be an appropriate alternative to VATS, and is associated with improved outcomes compared with open thoracotomy’.