
Child is not simply a miniature adult. Hence, surgery in paediatric age group is a specialised field involving correction of congenital defects so as to restore the normal anatomical and physiological function, which is best accomplished with trained paediatric surgeons, paediatric anaesthetist and support staff qualified for giving special care. Here’s a brief discussion on some common paediatric surgical problems.
Circumcision
Circumcision remains one of the commonest surgical procedures requested by parents. As a result of the incomplete separation of the epithelial layers during gestation and after birth, the prepuce (foreskin) may not be fully retractable until several years after birth. This is physiological phimosis and needs no treatment. However, there may be recurrent balanoposthitis resulting in narrowing of the prepuce which may require surgical correction.
Nowadays, preputioplasty has become an alternative surgical procedure to circumcision, especially in cases where surgery is deemed necessary on medical grounds. Preputioplasty releases the narrowed preputial opening without sacrificing the prepuce itself.
Undescended Testis
The recommended age for orchiopexy has decreased over the past several decades. Several clinical and histologic findings suggest the benefit of early therapy in improving fertility.
In cryptorchid testes, the number of spermatogonia per tubule and the seminiferous diameter is higher in boys under the age of one year. Hence, the present recommended age for surgery is between eight months to one year of age.
However, children who have a symptomatic hernia associated with a testicular undescend are advised surgery at the earliest to avoid the potential risk of torsion or irreducibility.
Hirschsprung’s Disease
One needs to rule out the possibility of Hirschsprung’s disease (congenital aganglionic megacolon) in a case of chronic constipation, especially if the symptoms are present since birth. Traditional treatment options for a child with Hirschsprung’s
disease included colostomy, followed by a definitive pull-through of the ganglionic bowel, and finally closure of colostomy. In this approach the child is subjected to three surgeries and is left with a scarred abdomen.
However, we now have the option of endorectal pull-through, a scarless surgery. Endorectal pull-through entails removal of the diseased aganglionic colon entirely by the endorectal route, and thus, the child’s abdomen remains untouched.
Video-Assisted Thoracoscopic Surgery (VATS)
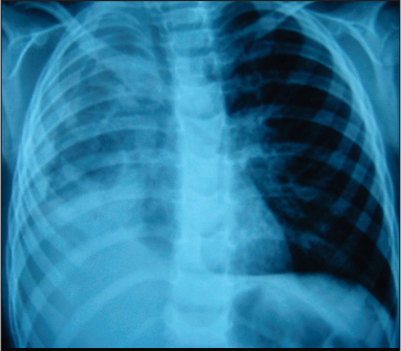
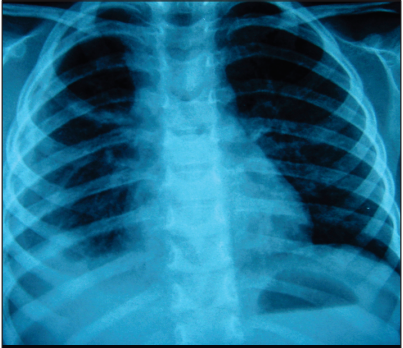
VATS is commonly used in the treatment of early thoracic empyema to release the fibrinous peel encasing the lung parenchyma (Fig: 1 & 2). However, its conversion to open thoracotomy is more frequent in chronic empyema cases. Hence, the patients of empyema should be identified in the early stages so as to avoid a thoracotomy.
Multi Stage vs Single Stage Surgery
Conventionally, the treatment for correction of congenital anomalies would entail a staged approach, whereby the child had to undergo multiple surgeries. However, with improved expertise and advanced infrastructure, today we are in a position to offer single stage reconstruction for most of the congenital anomalies.
At Kokilaben Hospital, we also have antenatal screening for detecting the anomalies in the unborn child under the guidance of our Advanced Foetal Care Unit (AFCU) team. Initial evaluation by a Foetal Medicine Specialist will assist in the detection of foetal anomalies during gestation, thus helping in early and accurate management of the case.