Patients with acute myocardial infarction need to reach an appropriate hospital facility within the shorteswt possible time for prompt, well-managed treatment and to ensure the best outcome
Chest pain management continues to be a challenge to hospitals. Often, treatment gets delayed due to a variety of reasons. Many examples can be cited where patients with non-cardiac chest pain have been hospitalised, investigated and traumatised, to end up as cardiac neurotics. On the other hand, many cases of cardiac ischaemia with normal ECG have been sent back, only to collapse and die at home. In these cases, the golden early hours of treatment are missed and the patients eventually suffer severe damage to their left ventricle. It is therefore essential to have clear guidelines regarding management of the various presentations of acute myocardial infarction.
Chest Pain and normal ECG at time of presentation:
6% Risk of developing ST Elevation MI
15% Risk of Non-ST Elevation MI
Importance of Troponin
Highly sensitive for myocardial necrosis Rise after four to six hours Peak at 24 hours Remain positive for 10 to 15 days False positive can occur with:
- Myocarditis
- Renal failure
- Pulmonary embolism
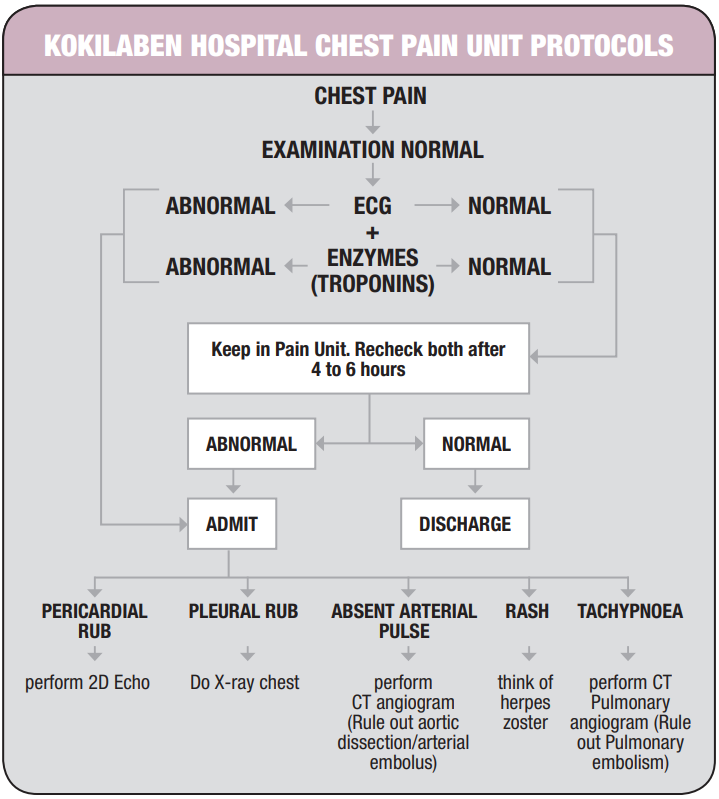
Kokilaben Hospital has set up a special Chest Pain Unit in the hospital’s emergency department which works according to strict protocols. This helps in the prompt institution of treatment and avoids unnecessary ICU admission.
When a patient is admitted with chest pain to our Chest Pain Unit, a detailed history is taken, and physical examination is performed, followed by an ECG. If the examination shows a pericardial or pleural rub or herpes, appropriate investigations are performed and required treatment started. If ECG shows ST elevation, prompt treatment with thrombolysis is initiated or the patient is sent to the cardiac catheterisation laboratory for primary coronary angioplasty. If ECG shows ST depression, the patient is sent to ICU and Troponin values are measured. If the values are high, early angiography is advised; but if the values are normal, conservative treatment is continued.
If the initial ECG is normal in the pain unit, Troponin values are sent and patient kept in the unit for observation. If the Troponins are raised, he/she is admitted to ICU and treated as unstable angina. If Troponins are normal, then both the ECG and Troponins are rechecked after four to six hours. If found normal again, and the patient is comfortable, he/she is sent home and called for a planned stress test. If either test results are abnormal, after the second testing, he/she is admitted to the ICU.
MBCPK (Creatine Phosphokinase–MB) can also be measured if Troponins are not available; however, they are less sensitive than Troponins and are raised later and therefore less useful. They can help judge the size of the myocardial infarction.
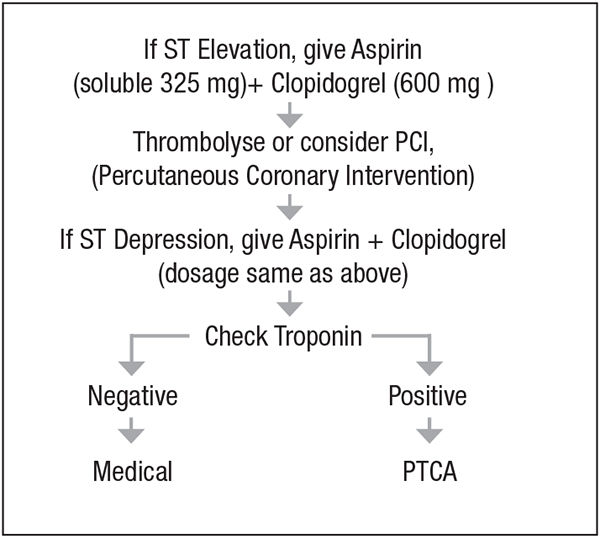
Patients with myocardial infarction need early administration of 325 mg of soluble aspirin (not enteric coated) and Clopidogrel as a loading dose of 600 mg for rapid anti-platelet effect. If thrombolysis is performed, it is started immediately to ensure rapid arterial recanalisation.
Kokilaben Hospital’s Chest Pain Unit follows these protocols which are now standard procedures across most international hospitals . This Unit is led by a team of experienced full-time consultants who provide immediate and undivided attention to these patients, thus ensuring better management and optimum results.
Special Tests
- Nuclear Testing
Hand-held probes with technitium SCAN—Cold Spot suggestive of MI can be detected in the chest unit and aid in diagnosis of borderline cases. - CT Coronary Angiography
A new modality that is very good for quick and fairly accurate diagnosis of coronary anatomy. If normal, it is very specific for ruling out ischemia. However, it is costly and needs contrast injection and causes radiation exposure. - MRI
may be useful in some cases to detect an MI, but the cost and need to shift the patient makes it impractical.
Therapy for Chest pain with Abnormal ECG