
Congenital Heart Disease (CHD) is the most common birth defect and is a leading cause of deaths in the first month of life. The incidence of CHD is nearly 1 in 100 newborns. Surgery was the only treatment option until 1981 when a stenosed pulmonary valve was ballooned in the cardiac catheterisation laboratory, thus starting the era of Therapeutic Interventional Cardiac Catheterisation in CHD.
TABLE-1: INTERVENTIONS IN NEONATES
| Anomaly | Treatment of Choice |
| Aortic Valve Stenosis | Transcatheter Balloon Valvoplasty (Age & weight are not barriers) |
| Pulmonary Stenosis | Transcatheter Balloon Valvoplasty |
| Coarctation of the Aorta (COA) | Surgical Resection of the Coarctation followed by End to End Anastomosis. Balloon Angioplasty of the coarctation can be carried out as a bail out procedure |
| Duct Dependant Pulmonary Circulation | Blalock-Taussig (BT) Shunt: (Aorta to pulmonary artery shunt) A stent in the Patent Duct can be deployed in certain cases instead of the BT shunt |
| dextro-Transposition of the Great Arteries (d-TGA) | Transcatheter Balloon Atrial Septostomy widens the Atrial Septal Defect thereby improving saturation. An arterial switch is the curative surgery performed in the neonatal age |
TABLE-2: INTERVENTIONS IN INFANTS AND OLDER CHILDREN
| Anomaly | Treatment of Choice |
| PDA Closure | Transcatheter Closure using an umbrella device or coil |
| ASD Closure | Transcatheter Closure (Fig-1) using an umbrella device is possible in most secundum type of ASDs. Primum and sinus venosus ones have to be closed surgically |
| VSD Closure | Surgical patch closure is performed. Transcatheter Closure using an umbrella device is possible in a few cases |
| Aortic or Pulmonary Stenosis | Transcatheter Balloon Valvoplasty (As in Table-1) |
| Pulmonary Artery Stenosis | Transcatheter Angioplasty |
| Coarctation | Transcatheter Balloon Angioplasty + Stent is as effective as surgery |
| Miscellaneous Conditions | Aorto-pulmonary collaterals and fistulae can be closed by the transcatheter route |
OUR SUCCESS STORIES
Children’s Heart Centre team has successfully balloon dilated a 1.7 kg neonate with critical aortic stenosis. Valve dilatation was carried out with an appropriately sized balloon catheter introduced from the femoral artery. The baby was discharged home two days later. The baby is now two months old and thriving.
A neonate with pulmonary atresia underwent successful stenting of his ductus with a 3.5 mm coronary stent one month ago. He is doing well on his first follow up.
In the past two years, 15 neonates with critical aortic valve stenosis have been treated with balloon valvuloplasty with success rate similar to the centres across the world.
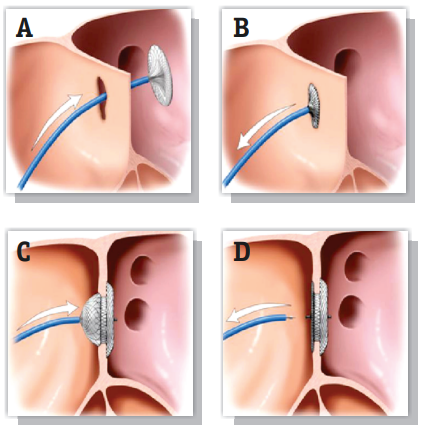
Fig 1: The ASD Occluder Device being placed across the atrial septum
Surgeries described in the above tables are conducted in our hospital to correct different heart defects in children. However, in certain situations, the surgeon and the cardiologist work together. The setting may be a baby with hypoplastic left heart syndrome or complex Tetralogy of Fallot or a sick infant with a large muscular VSD. The hybrid procedures highlight the inherent cohesiveness of every successful paediatric cardiac team.